This blog evaluates the potential for unanticipated Adverse Events (AEs) in children >2 years of age.
The one aspect of pediatric drug development which is a major concern is drug safety. While children, at exposures similar to those in adults, will likely have the same AEs as adults, it is also possible they may have AEs not seen in adults. These latter AEs, many of which were initially ascribed to the non-specific ‘immaturity’ of the child, were later re-assigned to a more specific developmental PD or off-target effect. Nevertheless, until such time the developmental PD and potential off-target effects are completely known, there will always be AEs uncovered in studies in children that relate to immature organ systems.
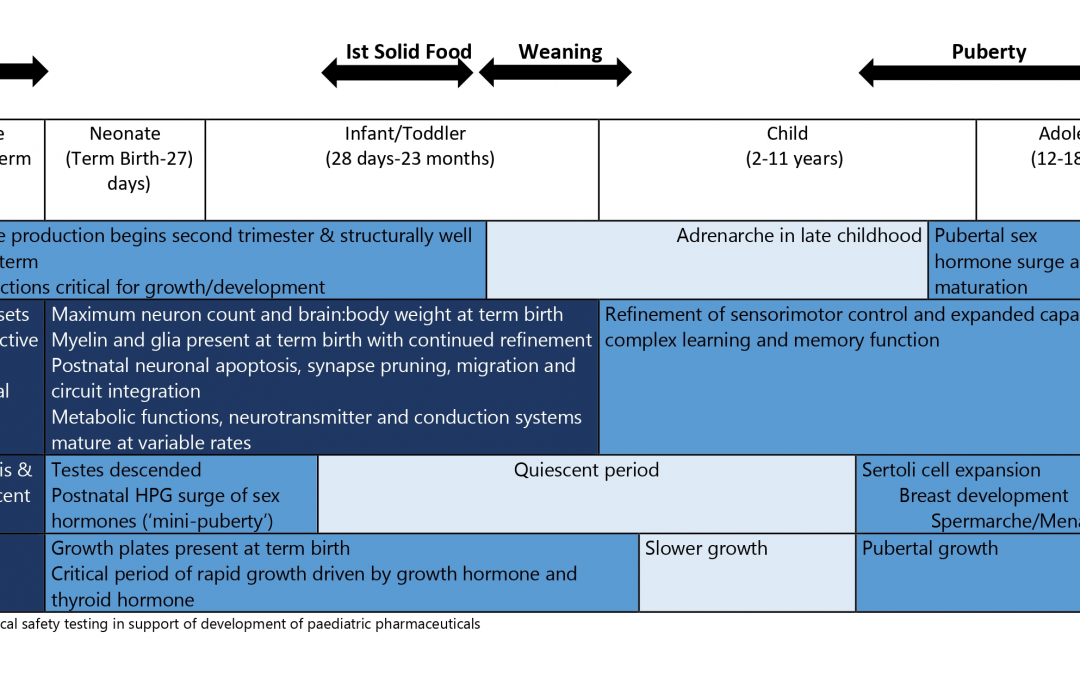
As can be seen from the tabular representation, the critical and active period of structural and functional maturation is completed by the age of two years for most organ systems, barring a few. Here we identify organ systems that need to be monitored closely for AEs in children >2 years.
The endocrine, reproductive and skeletal systems complete their initial critical and active period of maturation by age two and have a second critical period around pubescence. The onset of pubescence is variable with girls in general achieving pubescence earlier than boys. The actual age of onset of pubescence may also differ significantly within the same gender. In general, when evaluating drugs in children around pubescence, it is good to incorporate elements such as Tanner Sexual Maturity Rating Score, and growth charts (height, upper and lower segment ratios) into the safety assessments. Valproic acid (hyperandrogenism) and tetracyclines (deposition in bones and teeth) have AEs unique to these organ systems.
The nervous system is unique in that, while the critical period of maturation may be considered completed by the age of two years, the active period of maturation continues until the age of about 18 years. In the central nervous system (CNS), the main steps of maturation consist of neuronal proliferation, migration, organization and myelination. Proliferation of astrocytes and glia are completed in-utero. The neurons thereafter migrate and differentiate – a process wherein dendritic formation and axon formation begin. Synaptogenesis is 50% complete at age two and by four years it is nearly 100% complete. Neurotransmitter system maturation is complete by three years. Myelination, which begins at birth, is the last to end. Clinical trials in children beyond two years of age need to monitor closely for AEs related to the CNS. Monteleukast has been associated with neuropsychiatric events; anti-histamines with paradoxical excitation; phenobarbital with paradoxical restlessness, over activity; topiramate with oligohydrosis and hyperthermia.
Overall, the pediatric population > 2 years of age is likely to have the same AE profile as adults at similar exposures, with the exception of organ systems that may be considered as immature.
For an overview on pediatric drug development, please read our blog Pediatric Drug Development: Four Critical Considerations
For more blogs, please visit: https://www.rxmd.com/insights